Introduction
Uterine fibroids, also known as leiomyomas, are benign tumors that develop within or on the uterus. Although fibroids can appear in any person with a uterus, Black women in particular face disproportionately high rates of occurrence, earlier onset, and more severe symptoms.
Despite this well-documented disparity, fibroids in Black women frequently go unaddressed—or are dismissed outright—in medical settings, leading to challenges such as heavy bleeding, chronic pain, and potential fertility complications.
This article explores the reasons behind their prevalence in Black women, the social and medical factors that perpetuate neglect, and potential solutions for better health outcomes.
Understanding Uterine Fibroids
What Are Fibroids?
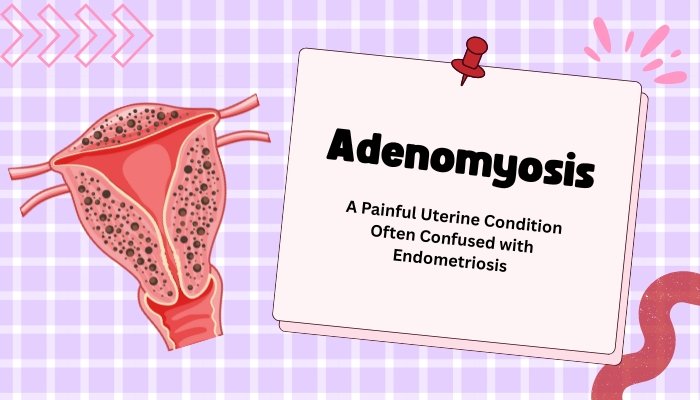
Fibroids are noncancerous growths arising from the muscle tissue of the uterus. They range in size from tiny, undetectable nodules to masses large enough to distort the uterine shape. Most fibroids are classified based on their location:
- Intramural: Embedded within the uterine wall.
- Submucosal: Protruding into the uterine cavity, often causing heavy menstrual bleeding and fertility issues.
- Subserosal: Extending outward from the uterus, occasionally pressing on surrounding organs.
While fibroids are generally benign, they can trigger significant symptoms—particularly if they grow large or numerous.
Common Symptoms
- Heavy or Prolonged Menstrual Bleeding: Leading to anemia and fatigue.
- Pelvic Pain or Pressure: Chronic discomfort can radiate to the lower back or legs.
- Frequent Urination: If fibroids press against the bladder.
- Reproductive Challenges: In some cases, submucosal fibroids can impede implantation or pregnancy, though many conceive successfully.
However, many fibroids remain asymptomatic, only discovered incidentally during a routine pelvic exam or ultrasound.
Why Are Fibroids More Common in Black Women?
Higher Prevalence and Earlier Onset
Research repeatedly shows that Black women are:
- Three to Four Times More Likely to develop fibroids than women of other racial backgrounds.
- More prone to being diagnosed at younger ages—sometimes in their 20s, whereas diagnoses for other groups may peak in their 30s or 40s.
- Likely to experience larger and more numerous fibroids, intensifying painful periods, pelvic pressure, and potential complications.
Potential Contributing Factors
- Genetic Predisposition
- Some studies suggest particular genetic markers or family history patterns that predispose Black women to fibroid formation.
- Hormonal Influences
- Estrogen and progesterone seem to encourage fibroid growth. Subtle differences in hormone metabolism or receptors might amplify fibroid susceptibility.
- Environmental and Lifestyle Exposures
- Stress, obesity, dietary patterns, or hair relaxers are studied in relation to fibroid risk, though conclusive evidence remains mixed.
- Vitamin D Deficiency
- Vitamin D may play a protective role against fibroids. Higher deficiency rates, seen more frequently in Black populations due to melanin impacting sunlight absorption, could be a piece of the puzzle.
While these elements help explain patterns, the precise causes of fibroids—and why they’re so prevalent in Black women—remain an active area of research.
Neglect in Diagnosis and Treatment
Delayed or Dismissed Symptoms
Many Black women recount how heavy bleeding or severe cramps are minimized as “normal period pain,” despite obvious red flags like debilitating discomfort or anemia. Medical professionals might misattribute complaints to stress or downplay them if fibroids are not initially suspected.
Healthcare Inequities and Distrust
- Implicit Bias: Studies show that African American patients sometimes receive less aggressive pain management or are not taken as seriously when reporting symptoms.
- Lack of Access: Neighborhoods with fewer specialized gynecological services limit timely ultrasounds or advanced procedures.
- Historical Context: Mistrust toward healthcare systems, shaped by historical injustices, may deter some from seeking repeated second opinions or recommended follow-ups.
Consequences
When left untreated, fibroids can grow, increasing the likelihood of severe anemia, fertility problems, or major surgeries like hysterectomy that might have been avoidable with earlier intervention.
Treatment Options and Barriers
Medical Management
- Medications:
- Hormone Therapies (GnRH agonists, birth control pills) help shrink fibroids or manage bleeding, though side effects can be significant.
- Tranexamic Acid/NSAIDs to reduce heavy menstrual flow and pain.
- Uterine Artery Embolization (UAE): Minimally invasive approach where particles block blood flow to fibroids, causing them to shrink.
Surgical Interventions
- Myomectomy: Surgical removal of fibroids, preserving the uterus. This is often favored if future fertility is desired.
- Hysterectomy: Removing the uterus is definitive for fibroid elimination, but it ends reproductive capability. Sometimes recommended when fibroids are extensive or other methods fail.
Financial and Informational Obstacles
- Insurance Coverage Gaps: Some advanced procedures like MRI-guided focused ultrasound might not be covered, limiting less invasive solutions.
- Limited Provider Familiarity: Not all gynecologists are equally trained in advanced fibroid treatments (e.g., laparoscopic myomectomy or specialized uterine-sparing techniques).
- Informed Decision-Making: Without accessible or culturally aware counseling, many Black women might default to more drastic surgeries, not realizing less invasive alternatives exist.
Empowering Patients and Improving Care
Advocacy and Education
- Patient Support Groups: Online communities and local fibrodis advocacy organizations facilitate resource sharing, from self-care tips to surgeon recommendations.
- Public Health Campaigns: Emphasizing that “heavy periods” or extreme cramps should be medically evaluated, especially if interfering with daily activities or causing anemia.
Cultural Competence in Healthcare
- Training and Awareness: Healthcare providers can address implicit biases, ensuring Black women’s complaints are given thorough attention and that fibroid screening is standard when indicated.
- Community Engagement: Partnerships with churches, nonprofits, or local influencers can normalize discussions on menstrual health, encouraging early medical consultations.
Expanding Research
- Gene-Based Studies: Investigating specific genetic and epigenetic contributors might point to novel therapies or prevention strategies.
- Inclusion in Clinical Trials: Prioritizing minority recruitment ensures results reflect the full fibroid-affected population, guiding tailored interventions.
Self-Care and Lifestyle Strategies
Diet and Exercise
- Maintaining Healthy Weight: Excess adipose tissue can influence hormone production, exacerbating fibroid growth.
- Anti-inflammatory Foods: Fruits, vegetables, and lean proteins can help minimize some hormone-driven processes.
- Stress Management: Chronic stress might disrupt endocrine balance, so practices like yoga or meditation could indirectly help.
Regular Checkups
- Annual Gynecological Exams: Early detection of fibroid growth can open the door to less invasive interventions.
- Monitoring Symptoms: Keeping a journal of menstrual flow, pain levels, or changes can clarify patterns for timely physician visits.
Conclusion
While uterine fibroids occur in individuals of all backgrounds, Black women face disproportionate rates, along with cultural, medical, and socioeconomic barriers that amplify harm. From overlooked symptoms to underutilized advanced therapies, the gap in care can result in avoidable complications. However, a rising tide of advocacy, combined with better education and clinically advanced interventions, is reshaping this narrative. By ensuring equitable research funding, training healthcare professionals to appreciate and address specific community needs, and championing public dialogue around fibroids, Black women can secure early, effective, and respectful treatment.
Ultimately, bridging these gaps not only alleviates personal suffering but also fosters a healthcare environment where all people with uterine fibroids receive appropriate, informed, and empathetic care.
References
-
- Eltoukhi HM, Modi MN, Weston M, Armstrong AY, Stewart EA. The health disparities of uterine fibroid tumors for African American women: a public health issue. Am J Obstet Gynecol. 2014.
-
- Stewart EA, Laughlin-Tommaso SK, Catherino WH. Epidemiology of uterine fibroids. Fertil Steril. 2017.
-
- Cardozo ER, Clark AD, Banks NK, et al. The impact of fibroids on fertility: Ebony or Ivory? Fertil Res Pract. 2020.